Covid transmission
Improving ventilation will help curb SARS-CoV-2
There has been a misunderstanding about how the virus spreads

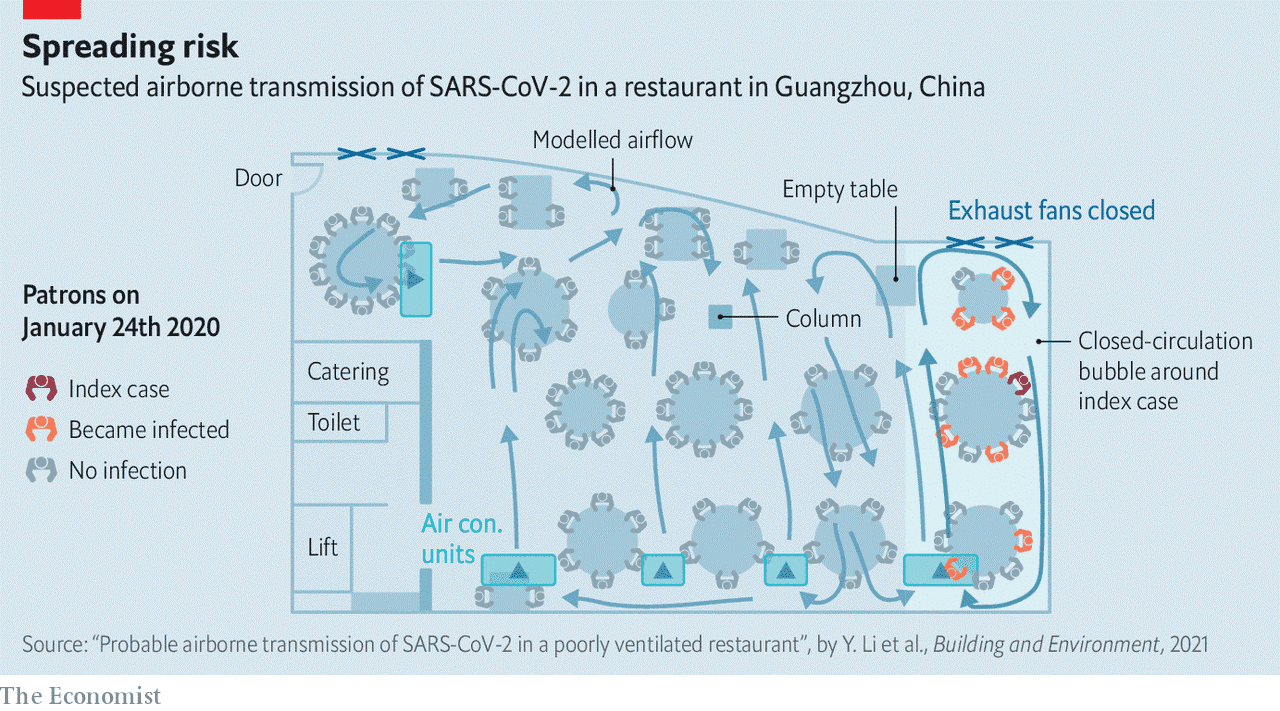
On january 24th 2020 three families, together numbering 21 people, came independently to eat lunch at a restaurant in Guangzhou.
It was the eve of the Chinese New Year.
Extra seating had been squeezed in to accommodate more patrons than usual, and these families were crowded onto neighbouring tables along one wall of the windowless room (see plan).
The largest of them—a party of ten who had arrived the day before from Wuhan—sat around the middle table.
Later that day, one of their number developed fever and a cough and, at a hospital, was diagnosed with covid-19.
Within two weeks, ten of the 21 were confirmed as being infected with sars-cov-2.
The families involved had never met and video footage showed they had no close contact during the lunch.
An initial analysis by the Guangzhou Centre for Disease Control and Prevention proposed that the infection had spread via respiratory “droplets”.
But medical lore has it that such droplets—defined as particles expelled while breathing that are more than five microns across—cannot travel more than a couple of metres after they have been exhaled.
And some of those who became infected during the lunch were farther than that from the “index” patient.
It made no sense.
How could a single infected person transmit the virus to nine others in just an hour when there had been no direct contact between them?
Current thinking
The outbreak at the Guangzhou restaurant was the first recorded “superspreading” event of the pandemic.
Superspreading is loosely defined as being when a single person infects many others in a short space of time.
More than 2,000 cases of it have now been recorded—in places as varied as slaughterhouses, megachurches, fitness centres and nightclubs—and many scientists argue that it is the main means by which covid-19 is transmitted.
In cracking the puzzle of superspreading, researchers have had to re-evaluate their understanding of sars-cov-2’s transmission.
Most documented superspreadings have happened indoors and involved large groups gathered in poorly ventilated spaces.
That points to sars-cov-2 being a virus which travels easily through the air, in contradistinction to the early belief that short-range encounters and infected surfaces were the main risks.
This, in turn, suggests that paying attention to the need for good ventilation will be important in managing the next phase of the pandemic, as people return to mixing with each other inside homes, offices, gyms, restaurants and other enclosed spaces.
It has taken a long time for public-health experts to acknowledge that covid-19 routinely spreads through the air in this way.
Social distancing and mask-wearing were recommended with the intention of cutting direct, close-range transmission by virus-carrying droplets of mucus or saliva breathed out by infected individuals.
The main risk of spreading the illness indirectly was thought to come not from these droplets being carried long distances by air currents, but rather by their landing on nearby surfaces, on which viruses they were harbouring might survive for hours, or even days.
Anyone who touched such an infected surface could then transfer those viruses, via their fingers, to their mouth, eyes or nose.
This makes sense if sars-cov-2 spreads in the same way as influenza—which was indeed the hypothesis in March 2020, when the World Health Organisation ( who) declared the start of the covid-19 pandemic.
Hence the advice to disinfect surfaces and wash hands frequently.
Doctors did know at the time that not all respiratory particles fall fast.
Those smaller than five microns can become aerosols, staying aloft for hours and potentially travelling much farther than droplets, or simply accumulating in the air within a closed room.
Anyone inhaling these aerosols could then become infected. But this was assumed not to matter, because aerosols were thought to be relevant only in specialist medical settings, such as when patients are attached to a ventilator in an intensive-care unit. Intubation, as this process is known, does indeed create aerosols, as the breathing tube is forced down a patient’s trachea.
But a wider risk was not perceived. The who therefore played down the risks of aerosols, issuing guidance via its Twitter and Facebook pages at the end of March 2020 that the general public need not worry.
“FACT: #COVID19 is NOT airborne,” it said, adding that any claims to the contrary were “misinformation”.
Physics envy
Researchers outside the medical world, however—especially those who study the physics of particles in the air—felt the evidence pointed in a different direction.
The Guangzhou restaurant outbreak was an early warning.
Around the same time, 1,300km across the country in Ningbo, 23 of 68 passengers on a bus fitted with an air-recycling system had been infected during a one-and-a-half-hour journey.
But the worst known case of superspreading early in the pandemic was American. This happened at a choir practice in Skagit Valley, Washington State, in March 2020.
Of the 61 people present during a two-and-a-half-hour meeting, 53 became infected.
In all these cases, investigation showed that those infected were not necessarily the people closest to the index patients, as might be expected if transmission had been by droplet or surface contact.
None of this surprised Lidia Morawska, a physicist at the Queensland University of Technology, in Brisbane, Australia.
She had spent much of her career studying how pollution caused by so-called particulate matter, such as dust and smog, affects air quality.
After the original sars outbreak, which happened in 2003, she began experiments to show how respiratory particles are generated in people’s throats and then transported through the air.

She demonstrated that received medical wisdom is wrong.
Because exhaled breath is a moist, hot, turbulent cloud of air, a five-micron-wide droplet released at a height of one and a half metres (about the distance above ground of the average mouth or nose) can easily be carried dozens of metres before settling.
Also, the generation of respiratory particles is not restricted to medical settings.
Liquid drops of all sizes—including those defined as aerosols—are continuously shed while people are breathing, talking, sneezing or singing (see chart).
In July 2020 Dr Morawska wanted to bring this work to the attention of public-health agencies.
She assembled a group of 36 experts on aerosols and air quality to write an open letter outlining their evidence for infection by smaller liquid drops and calling on the who to change its tune on airborne transmission.
“We appeal to the medical community and to the relevant national and international bodies to recognise the potential for airborne spread of coronavirus disease 2019 (covid-19),” they wrote in Clinical Infectious Diseases.
“There is significant potential for inhalation exposure to viruses in microscopic respiratory droplets (microdroplets) at short to medium distances (up to several metres, or room scale), and we are advocating for the use of preventive measures to mitigate this route of airborne transmission.”
More than 200 other researchers from 32 countries also signed the letter.
One signatory was Jose-Luis Jimenez, an atmospheric chemist at the University of Colorado, Boulder.
He says that the confusion in health circles over whether or not airborne transmission of sars-cov-2 is important can be traced back to medical textbooks that still contain outdated descriptions of how respiratory particles are produced and move.
But the widespread assertion, still stubbornly promulgated by the who, that droplets above five microns in diameter do not stay airborne, but rather settle close to their source, is a dodgy foundation on which to build public-health advice.
According to Dr Jimenez, physicists have shown that any particle less than 100 microns across can become airborne in the right circumstances.
All of this matters because hand-washing and social distancing, though they remain important, are not enough to stop an airborne virus spreading, especially indoors.
Masks will help, by slowing down and partially filtering an infectious person’s exhalations.
But to keep offices, schools, hospitals, care homes and so on safe also requires improvements in their ventilation.
Fan-tastic
Under pressure from physicists, the who recently acknowledged that better ventilation should be used to help prevent covid-19’s spread—and in March it published a “roadmap” to that effect.
But the document fell far short of properly recognising the hazard of airborne transmission and, therefore, the need to control it.
Despite overwhelming evidence that it happens, the agency still maintained that sars-cov-2 “mainly spreads between people when an infected person is in close contact with another person”.
Others, though, are acting on the new knowledge.
Martin Bazant, a chemical engineer, and John Bush, a mathematician, both at the Massachusetts Institute of Technology, have devised a way to calculate how long it would be safe to stay within a room that contains an infected person.
The pair described their model in a paper in a recent issue of the Proceedings of the National Academy of Sciences.
Applied to a typical American school class of 19 pupils and a teacher, the safe time after an infected individual enters a classroom that is naturally ventilated (that is, how long before the risk of infection is unacceptably high) is 72 minutes.
This period can, though, be extended in two ways.
One is by mechanical ventilation of the room, which increases the safe time to 7.2 hours.
The other is by everyone wearing masks.
In the absence of mechanical ventilation, mask-wearing increases the safe time to eight hours.
But the real benefit comes from combining these approaches.
That pushes the safe time up to 80 hours—almost 14 days if a school day is six hours long.
Add in intervening weekends and a class wearing masks in a school room with adequate ventilation would thereby be safe for longer than the time it takes to recover from covid-19, which is typically between one and two weeks.
School transmissions would thus be rare.
A caveat is that the modelling assumed a classroom with minimal talking, physical activity or singing by the pupils.
But games lessons would usually be outdoors and singing lessons could be.
As to too much talking, teachers might welcome an unimpeachable reason to tell pupils to keep quiet in class.
Infection risk will not always be distributed evenly around a room.
Jiarong Hong, a mechanical engineer at the University of Minnesota, Minneapolis, therefore used computer models to study how aerosols would spread in a classroom, according to the location of an infected individual and the position of nearby fans or air filters.
Assuming the teacher was infected, and so was releasing virus-laden aerosols at the front of the class, Dr Hong’s modelling shows that placing an air cleaner or extractor fan at the front of the room sets up an airflow which prevents the movement of such aerosols towards the pupils.
An even better aerosol-cleansing effect is achieved when the fans and filters are elevated above the people in the room.
This takes advantage of the rising air plumes created by body heat, which mean that exhaled aerosols tend to float upwards.
Dr Hong’s modelling shows that even small, cheap box fans mounted in this way would do a good job of keeping classrooms safe and preventing aerosols from building up to dangerous levels.
Dr Hong has also modelled the air flow in the Guangzhou restaurant outbreak of January 2020. As the plan shows, he found that the movements of virus-laden aerosols around the three affected families of diners matched the seating positions of the people who eventually became sick. The outbreak occurred because there was no source of external fresh air and a nearby recirculating air conditioner redistributed aerosols from the infected person to the other tables, creating a contaminated bubble of air that was increasingly burdened with viruses over the course of the lunch.
The risk, then, is real.
But how can the occupants of a room know whether it is well-ventilated?
Just because a room feels spacious and an air conditioner is operating does not mean the air inside it is clean.
Here, Dr Morawska has a suggestion.
In a (non-scientific) experiment last year, she took a carbon-dioxide meter into a large, high-ceilinged, air-conditioned restaurant near her home.
CO2 concentrations can be a useful proxy for clean air.
Outdoor air contains around 400 parts per million (ppm) of the gas, and people’s exhaled breath contains around 40,000ppm.
Exhaling into a room therefore gradually raises its CO2 concentration unless the ventilation is good enough to remove the excess.
According to experts on air quality, anything below 500ppm in a room means the ventilation is good.
At 800ppm, 1% of the air someone is breathing has already been exhaled recently by someone else.
At 4,400ppm, this rises to 10%, and would be classed as dangerous.
These sorts of levels are seen only in crowded spaces with poor airflow.
To keep the risk of covid-19 low, CO2 levels should be well below 700ppm.
When Dr Morawska conducted her experiment, the restaurant had ten people in it—far fewer than would normally be allowed—and the CO2 concentration was already 1,000ppm when she arrived. Within an hour it had jumped to 2,000ppm.
“We continued sitting during the dinner for another hour or so,” she says.
“So if there was someone infected there, well this could have been a problem.”

Though anecdotal, that tale indicates a serious risk—and one which resonates beyond covid-19.
All sorts of symptoms, from headaches, fatigue and shortness of breath to skin-irritation, dizziness and nausea, are linked to poor ventilation.
It has also been connected with more absences from work and lower productivity.
The ventilation measures needed to deal with all this are not difficult, but existing regulations and design standards often have different objectives—particularly, these days, conserving heat and thus reducing energy consumption.
That often means recirculating air, rather than exchanging it with fresh air from the outside world. (An exception is passenger aircraft, which refresh cabin air frequently.)
In situations where it is not possible to reduce health risks by ventilation alone—for example, places like nightclubs, where there are lots of people crowded together, or gyms, where they are breathing heavily—air filtration could easily be incorporated into ventilation systems.
Air could also be disinfected, using germicidal ultraviolet lamps placed within air-conditioning systems or near ceilings in rooms.
All change
And then there is public awareness.
“Before this pandemic it was completely socially acceptable to come to the office coughing, sneezing, spreading viruses around,” says Dr Morawska.
“No one would say anything—even people educated to understand how infections are transmitted.”
That insouciance must be corrected, she says.
The who must acknowledge the need to control airborne pathogens and governments must agree and enforce comprehensive standards for indoor air quality that keeps people healthy.
One way to ensure compliance might be to issue ventilation certificates for buildings, similar to the food-hygiene certificates which already exist for restaurants.
Occupants should also be given information about air quality routinely, she adds, through the use of monitors and sensors that can display a room’s carbon-dioxide levels or other relevant measures.
For new buildings this should not cost much extra, though replacing exiting ventilation systems might be costly.
But not as costly as covid-19 has been.
And if improvements in indoor air quality also reduced absenteeism and improved productivity, those gains might cover that cost.
“Although detailed economic analyses remain to be done,” wrote Dr Morawska in a recent edition of Science, “the existing evidence suggests that controlling airborne infections can cost society less than it would to bear them.”
0 comments:
Publicar un comentario